On June 12, 2025, the FDA granted approval for pembrolizumab (Keytruda) as a neoadjuvant and adjuvant therapy in adults with resectable, locally advanced head and neck squamous cell carcinoma (HNSCC), provided the tumour expresses PD-L1 with CPS ≥ 1.
This marks the first perioperative checkpoint inhibitor approval for resectable HNSCC
KEYNOTE-689: The Trial That Changed the Paradigm
Study Design & Patient Population
- Phase III, randomized, open-label global trial (NCT03765918)
- Enrolled 714 patients with stage III–IVA resectable HNSCC
- Stratified by PD-L1 CPS ≥ 1
- Randomization (1:1):
- Arm A: Neoadjuvant pembrolizumab → surgery → adjuvant pembrolizumab with radiotherapy ± cisplatin → pembrolizumab maintenance
- Arm B: Surgery → standard adjuvant radiotherapy ± cisplatin
Efficacy Results
- Primary endpoint: Event-free survival (EFS) in PD-L1 CPS ≥ 1 group
- Median EFS: 59.7 months (95% CI: 37.9–NR) vs 29.6 months (19.5–41.9) in control arm
- Hazard ratio (HR) = 0.70, p = 0.00140 → 30% risk reduction
- Major pathologic response (mPR) rates also significantly higher
Safety Profile
- Adverse effects consistent with known immune-related toxicities (pneumonitis, thyroiditis, colitis, etc.)
- No unexpected perioperative surgical delays
NIVOPOSTOP: Nivolumab in the Adjuvant Setting
The NIVOPOSTOP (GORTEC 2018-01) phase III trial (NCT03576417), tested adjuvant nivolumab (Opdivo), administered after surgery along with standard chemoradiotherapy.
Study Design & Population
- Enrolled ~680 high-risk resected HNSCC patients
- Compare: surgery → standard cisplatin + RT vs surgery → cisplatin + RT + nivolumab
Efficacy Results
- Primary endpoint: Disease-free survival (DFS)
- Three-year DFS: 63.1% with nivolumab vs 52.5% with SOC
- HR ≈ 0.76 (95% CI 0.60–0.98), p ~0.03 → ~24% relative improvement
- Nivolumab group had 63.1% DFS vs 52.5%; 1-year DFS 71.7% vs 64.7%, 2-year DFS 64.9% vs 56.2%
Safety & Tolerance
- Similar overall safety profile; however, grade 4 AEs higher in the nivolumab arm (13.1% vs 5.6%)—primarily neutropenia and lymphocytopenia
- Overall survival (OS) data immature but showing positive trend
Comparison & Clinical Implications
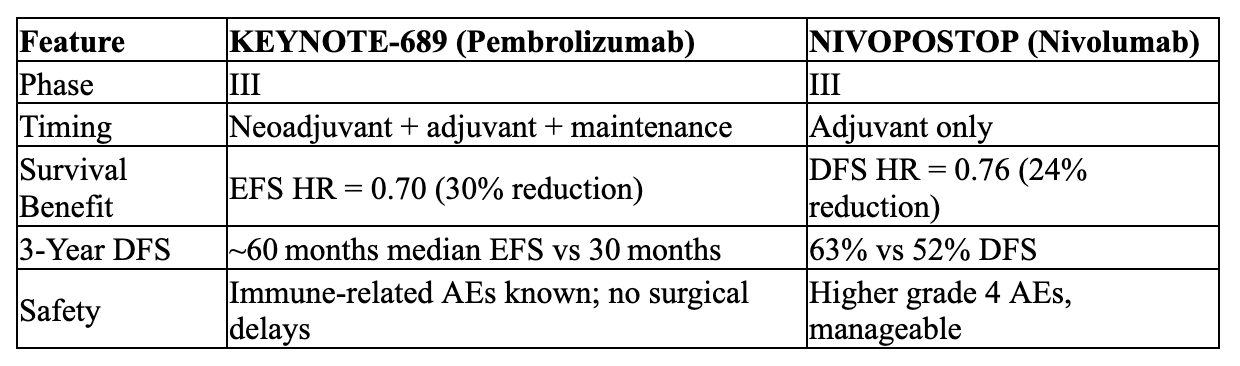
Both trials demonstrate the additive benefit of PD-1 blockade in perioperative HNSCC. KEYNOTE-689 leads the way with neoadjuvant immunotherapy, reshaping treatment paradigms in resectable disease. NIVOPOSTOP confirms postoperative nivolumab also offers a meaningful DFS advantage in high-risk patients, expanding options bolstered by ongoing OS data.
Looking Ahead
- FDA-approved regimen: KEYNOTE-689 sets a new standard—neoadjuvant and adjuvant pembrolizumab for PD-L1 CPS ≥ 1.
- Nivolumab: promising adjuvant role; broader FDA approval pending OS outcomes.
- Future research: revisiting sequencing (pre- vs post-op), combination strategies, biomarker refinement (PD-L1, mPR), and long-term OS data.
Summary
- Pembrolizumab now officially approved perioperatively in PD-L1+ resectable HNSCC after showing a dramatic 30% EFS reduction in KEYNOTE-689.
- Nivolumab, in the NIVOPOSTOP trial, improved 3-year DFS by ~24% as adjuvant therapy—a significant step toward expanding immunotherapy in this setting.
These breakthroughs herald a new era in curative-intent HNSCC treatment. If you’d like details on biomarker breakdown, surgical outcomes, economic impact, or practical clinical integration, join us at FaceInnovate 2025 in Dubai to discuss this paradigm shift in HNSCC management!


